

Introduction:
Adult T cell leukemia lymphoma (ATLL) is a rare T cell neoplasm caused by the human T-lymphotropic virus (HTLV-1) virus. Although there are indolent subtypes it is often a highly aggressive and chemotherapy refractory malignancy. We follow one of the largest cohorts in the United States and in this study, we sought to elucidate the prognostic factors associated with inferior survival.
Methods:
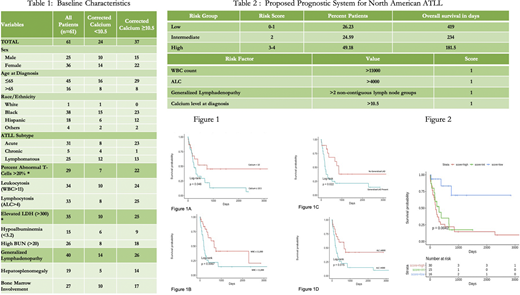
A retrospective analysis of patients diagnosed with ATLL at Montefiore Medical Center was conducted. Subjects included were censored at last point of contact. Variables collected included age, gender, race, ethnicity, ATLL subtype, white blood cell count (WBC), absolute lymphocyte count (ALC), corrected calcium level, lymphadenopathy (LAD) (two or more non-contiguous sites). Associations between WBC, ALC, corrected calcium level, LAD and median overall survival (mOS) were assessed using the Kaplan-Meier method with log-rank test. A four-point prognostic system was designed assigning one point to each: WBC > 11,000; ALC>4000; Corrected Ca≥10.5 and presence of LAD. Three risk groups were assigned based on the number of risk factors as follows: low (0-1 points), intermediate (2 points) and high (3-4 points) (Table 2). Association between these groups and OS was investigated using the Kaplan-Meier method with log-rank test.
Results:
A total of 61 ATLL subjects were included in this study (table 1). Hypercalcemia (Ca ≥10.5) was observed in 60.6% of subjects at diagnosis and was associated with inferior mOS (234 days) when compared to calcium < 10.5 (747days) (p=0.046), Figure 1A. WBC >11,000 had a strong association with inferior survival (175 days) compared to patients with a WBC ≤11,000 (666 days) (p= 0.0067) (Figure 1B). ALC > 4000 was also associated with inferior mOS (222 days) compared to ALC ≤4000 (666 days) (p=0.015) (Figure 1C). LAD was associated with mOS (188 days) compared with no LAD (847 days) (p=0.022) (Figure 1D). Based on these observations, we designed a prognostic system (0-4 points) (see above) to risk stratify newly diagnosed ATLL patients into: low (0-1 points), intermediate (2 points) and high (3-4 points) risk (Table 2). We divided our cohort into the above-mentioned risk groups and calculated their mOS. Kaplan Meier analysis (Figure 2) revealed a distinct mOS difference between the groups based on their risk score: Low: 419 days, Intermediate: 234 days and High: 181.5 days (p= 0.0042).
Conclusions:
We identify hypercalcemia (Ca≥10.5), leukocytosis (WBC> 11,000), lymphocytosis (ALC> 4000) and generalized LAD as poor prognostic factors in newly diagnosed ATLL. Using readily available information from basic laboratory and clinical parameters we propose a prognostic system to identify high risk individuals. Further validation will be needed using larger cohorts of this very rare disease.
Steidl:Aileron Therapeutics: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Stelexis Therapeutics: Consultancy, Current equity holder in private company, Membership on an entity's Board of Directors or advisory committees; Pieris Pharmaceuticals: Consultancy; Bayer Healthcare: Research Funding. Verma:stelexis: Current equity holder in private company; BMS: Consultancy, Research Funding; acceleron: Consultancy, Honoraria; Janssen: Research Funding; Medpacto: Research Funding. Janakiram:Takeda, Fate, Nektar: Research Funding. Shah:Celgene/BMS: Research Funding; Physicians Education Resource: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal